Incisional Hernia
Visit our YouTube channel | Mr Charles Leinkram
Incisional hernias occur at the site of a previous abdominal operation. The common types of abdominal operations which lead to incisional hernias are those for bowel surgery or gynaecological surgery. Others occur following stomach or gallbladder surgery and even at the entry site used for “key-hole” surgery, (i.e, the “port”).
It has been reported that after major abdominal operations, incisional hernias occur in up to 30% of cases. The reasons for this are that a long incision is made and the tissues are sutured together over an extensive area. Following major surgery there is often abdominal distension with gas or fluid, weakening of the tissues from infection or from excessive straining, e.g. vomiting or constipation. In addition, systemic factors such as poor nutrition, Diabetes or smoking also affect wound healing.
All of these factors may lead to a break down of the abdominal wound. This may occur very soon after surgery or even years later.
Mr Leinkram has developed a wide experience in repairing incisional hernias…
In his opinion, virtually all incisional hernias are anatomically different, and that their repair must therefore be tailored to suit the individual patient. We can illustrate this by showing some examples of incisional hernias that Mr Leinkram has repaired. However, before doing so, several general points need to be made:-
- We prefer to use the “open” method of repair, that is to make an incision on the abdomen.
- The hernia sac is opened and its contents are completely freed.
- The hernia sac is then excised.
- All adhesions to the abdominal wall are completely cleared.
- A large sheet of non-adherent mesh is securely stitched to the abdominal wall musculature using multiple transmuscular sutures.
- The abdominal wall muscles are then closed over the mesh.
- If there is a significant amount of associated skin laxity, this can also be excised, thus improving the cosmetic appearance, (see Case 4).
Mr Leinkram prefers the “open” method of incisional hernia repair over the alternative “key-hole” method because:-
- The hernia sac is excised completely.
- The mesh is securely sutured to the anterior abdominal wall musculature rather than being stapled or glued as is often done in the “key-hole” method. The mesh is therefore less likely to slip or become detached using the “open” technique.
- The muscle layer of the anterior abdominal wall can almost always be closed, thereby avoiding the creation of a “dead space”. A “dead space” can result in the accumulation of a significant amount of subcutaneous fluid post-operatively, giving rise the presence of a large swelling in the abdomen which can take weeks to resolve.
- The open method in effect constitutes a 2-layered closure of the hernia defect (an inner layer of the double-sided sheet of mesh, and a second layer of the closed muscle itself). In the key-hole method, only the placement of the inner layer is performed.
- The incisional hernia repair operation can also incorporate a “tummy-tuck” if required.
‘Rate My Doctor’ Patient reviews of Incisional Hernias performed by Mr Charles Leinkram:
1. “As a division 1 registered nurse l am very particular about who l choose when my family or l require surgery, so was pleased to be recommended by a trusted colleague to Mr Leinkram when l required an incisional hernia repair. Right from the initial consultation through to my hospital stay and post operative care l found Mr Leinkram and his team including the anaesthetist, physician, surgical assistant and office staff to be very pleasant and helpful to deal with and most of all extremely professional. Mr Leinkram is a highly experienced and very caring doctor with excellent communication skills. His lovely secretary Gill was more than helpful and explained everything to me thoroughly prior to my surgery, including all out of pocket costs, which l know as a nurse were very fair. Being a 49 year old woman l was very pleased to be able to have an abdominoplasty at the same time as my hernia repair and needless to say l am delighted with the outcome. Mr Leinkram did a fantastic job and l would highly recommend him to anyone, including my patients. The care l received from the staff at Mitcham Private Hospital was also of the highest standard. Thanks Mr Leinkram for all your wonderful care.”
2. “Went from North QLD to Victoria to have Charles repair an extremely large incisional Hernia after a very poor robotic prostatectomy operation using the Da Vinci system. Initially sought opinions from QLD surgeons and their knowledge and style of repair was dubious. Charles explained exactly what he would do and exceeded my expectations regarding the surgery and aftercare. Well worth the trip to see him and have him carry out the work. Surgeons staff were excellent and the hospital where it was done was equally as good.”
3. “My husband has had three surgeries with Mr Charles Leinkram, (2015), and each was undertaken with extreme professionalism and care. After a bad outcome from a hernia repair with another surgeon in 2014, Mr Leinkram had to remove and repair an infected hernia mesh, and to later surgically repair a much larger hernia (ventral hernia) following issues from the previous surgeon’s operation. At every step, my husband was asked to undertake tests to ensure all was well, and that there were no other issues. Thank God for Mr Leinkram’s tests as one of these revealed issues with my husband’s gall bladder which, after its removal, resulted in a significant diminution of reflux symptoms. Mr Leinkram’s receptionist Gill is equally caring and professional, as is the team he employs, for instance, Physician Dr Henry Voselis and others. OVERALL: My husband and I have no hesitation in recommending Mr Leinkram. His surgical skills and demeanor are excellent, and he surrounds himself with a team of caring and professional health professionals. We are so happy with everything. Please be aware that there are some modest out of pocket fees.”
(Source: https://www.ratemds.com/doctor-ratings/3639164/Dr-Charles-Leinkram-Melbourne-VIC.html)
Clinical Images
The case studies below contain clinical images. Click on the arrows to view the images.
Case 1.
Incisional hernia in a patient who had previously undergone vascular surgery for aorto-iliac disease.
Figure 1

Figure 2

Figure 2
Figure 3
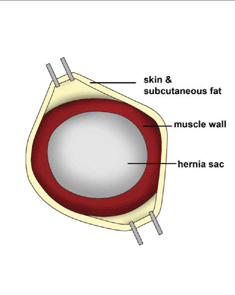
Figure 3
Figure 4
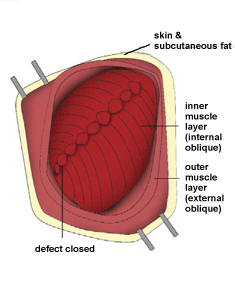
Figure 4
Figure 5
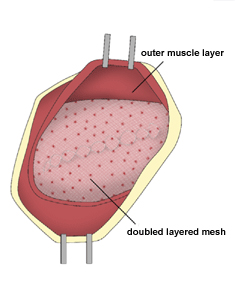
Figure 5
Figure 6
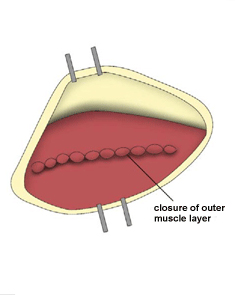
Figure 6
Figure 7

Figure 7
Figure 8

Figure 8
Figure 9

Figure 9
Case 2.
Incisional hernia in a patient who had previously undergone surgery for removal of a rectal cancer.
Figure 1

Figure 2

Figure 3
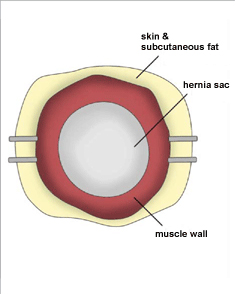
Figure 4
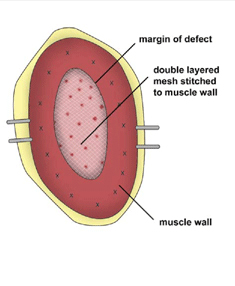
Figure 5
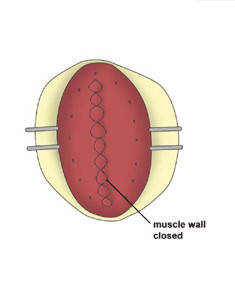
Figure 6
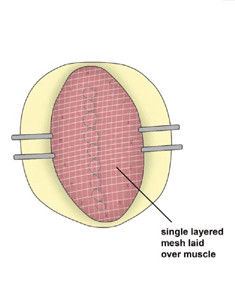
Figure 7

Figure 8

Case 3.
Incisional hernia in a patient who had previously undergone a cholecystectomy (removal of the gallbladder)
Figure 1

Figure 2

Figure 3
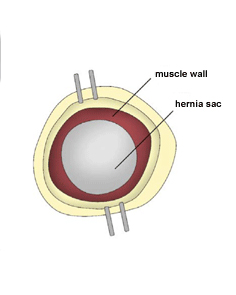
Figure 4
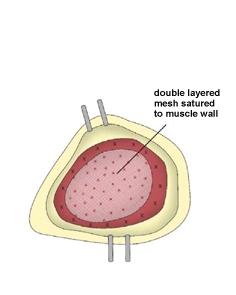
Figure 5
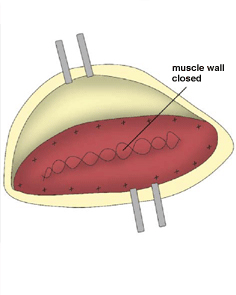
Figure 6
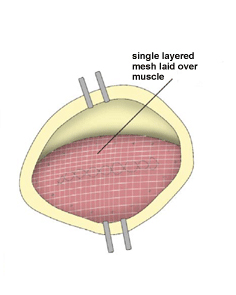
Figure 7

Figure 8

Case 4.
Incisional hernia adjacent to the umbilicus in a patient who had previously undergone key-hole surgery for removal of the gallbladder. An abdominoplasty (“tummy-tuck”) was also performed.
Figure 1

Figure 2

Figure 3
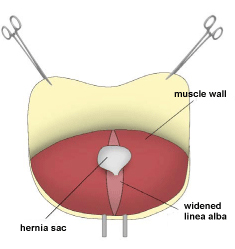
Figure 4
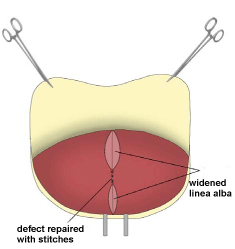
Figure 5
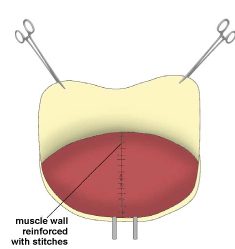
Figure 6

Figure 7

Case 5.
Recurrent incisional hernia in a patient who had previously undergone an attempted repair of this same problem. Prior to this, he had undergone multiple abdominal operations for complications following a key-hole umbilical hernia repair.
Figure 1

Figure 1
Figure 2

Figure 3
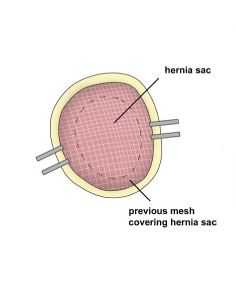
Figure 3
Figure 4
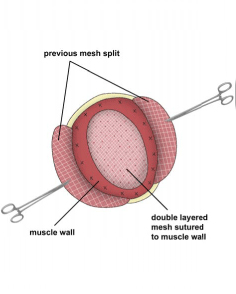
Figure 4
Figure 5
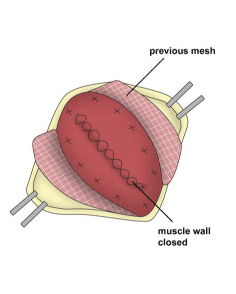
Figure 5
Figure 6
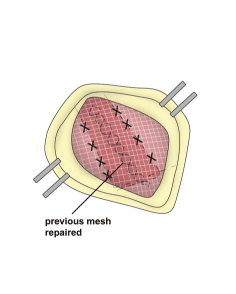
Figure 6
Figure 7

Figure 7
Figure 8

Figure 8